The Revenue Integrity Blind Spot
What if some of the revenue your practice has already earned is quietly slipping away without anyone noticing?
In most medical practices, revenue cycle discussions focus on visible challenges such as denied claims, delayed reimbursements, or aging accounts receivable. These issues are easy to identify and track, so they naturally receive the most attention. Yet another problem operates far more quietly in the background: insurance underpayments.
A claim may be approved and payment may arrive, creating the impression that everything worked as expected. But getting paid is not the same as getting paid correctly. In fact, hospitals absorbed an estimated $130 billion in Medicare and Medicaid underpayments in 2023, underscoring how reimbursement gaps can quietly accumulate across the healthcare system and affect provider revenue over time.
In this blog, we examine why insurance underpayments happen, where revenue leakage usually begins, and how high-performing practices are working to identify and recover these lost payments.
The Systemic Nature of Underpayments in Modern RCM
Insurance underpayments are often dismissed as occasional billing errors or isolated payer mistakes. In reality, they are a structural outcome of how modern reimbursement systems operate.
Across the industry, analysts estimate that providers lose approximately 1% to 3% of net patient revenue each year due to underpayments, a figure that can translate into significant financial loss for organizations operating on narrow margins. This leakage rarely stems from a single issue. Instead, it reflects the growing complexity of payer contracts and reimbursement policies.
Most payer agreements today contain multiple fee schedules, service-specific pricing rules, carve-outs, and location based reimbursement adjustments. These terms are then applied through automated adjudication systems that process claims at scale. As a result, payment calculations are influenced not only by CPT codes but also by modifiers, site of service rules, bundling logic, and policy edits embedded within payer systems.
This complexity creates an important distinction between denials, partial payments, and true contract variances. A denial is visible and triggers follow up. Partial payments may appear legitimate based on claim adjustments. Underpayments, however, occur when the allowed amount falls below the contracted rate without triggering a denial.
Because these calculations occur inside automated payer systems, underpayments are rarely random mistakes. They are the byproduct of reimbursement logic applied across millions of claims.
Where Revenue Leakage Actually Happens: An Operational Deep Dive
Insurance underpayments rarely stem from a single obvious mistake. In most cases, they reflect the common causes of revenue leakage in healthcare, emerging from small discrepancies embedded within the technical mechanics of payer reimbursement systems. Individually these differences may appear minor, but when they affect high volume services, the financial impact can compound quickly.
One common source of underpayment involves misloaded payer fee schedules. If contracted rates are entered incorrectly or an outdated version remains active within the payer system, claims may be reimbursed below the negotiated amount. Similarly, incorrect contract modeling within payer adjudication systems can produce discrepancies when reimbursement logic does not fully reflect the terms outlined in the payer agreement.
Errors can also occur through bundling logic and modifier pricing rules. Automated adjudication engines apply coding edits and modifier adjustments that sometimes suppress payment for services that should be reimbursed separately. Multiple procedure reduction calculations introduce another layer of complexity, particularly when payers apply reduction formulas that differ from contract language.
Operational factors add further risk. Site of service differentials, incorrectly priced carve out services, and mid-contract fee schedule updates that were never implemented can all influence the final allowed amount.
When these variances occur across frequently billed CPT codes, the effect is cumulative. Over thousands of encounters, even small reimbursement gaps can evolve into meaningful revenue leakage.
Why Most Practices Don’t Catch It
To understand why insurance underpayments go unnoticed, a natural question follows: Why do so many practices fail to detect underpayments in the first place?
The answer lies less in staffing and more in how most revenue cycle systems are designed. Payer contracts are often stored as static documents, frequently in PDF form, rather than translated into structured reimbursement logic at the CPT level. Without that modeling, it becomes difficult to compare what a payer actually reimbursed against what the contract requires.
Practice management systems add another limitation. These platforms are built to post payments and reconcile balances, not to validate reimbursement accuracy against contracted rates. Once a payment is posted and the claim is closed, the system typically treats the transaction as complete.
Meanwhile, billing teams are already focused on operational priorities such as claim submission, denial resolution, and payment posting. Variance analysis rarely fits into these workflows.
At the same time, many insurers rely on automated claim review systems that apply proprietary reimbursement logic tied to CPT codes and policy edits. Without deliberate payment verification, discrepancies can pass through unnoticed.
Financial Impact: Beyond the 1–3% Benchmark
Industry estimates often suggest that providers lose about 1 to 3% of net patient revenue to insurance underpayments each year. However, when broader revenue cycle inefficiencies such as denials, missed charges, and contract variances are included, total revenue leakage can rise to 7–11% or more, making it a far more significant financial risk than it initially appears. At first glance, this may appear manageable. In practice, however, even small percentage losses can translate into meaningful financial consequences.
For a medical practice generating ten million dollars in annual revenue, a two percent underpayment rate represents roughly two hundred thousand dollars in lost reimbursement. Because healthcare organizations typically operate on tight margins, this level of leakage can directly affect profitability, provider compensation, and long term financial stability.
Underpayments also distort financial visibility. When payment discrepancies go undetected, payer performance reports may suggest that contracts are performing as expected, even while reimbursement levels slowly decline. This weakens a practice’s negotiating position during contract renewals, since accurate variance data is often needed to challenge payer reimbursement trends.
There is also an operational cost. Practices that attempt to identify underpayments internally must allocate staff time to investigate discrepancies and pursue recovery. Many billing companies do not include this work within their standard service model, leaving providers to absorb the administrative burden.
The Strategic Shift: From Claims Processing to Payment Intelligence
As reimbursement complexity increases, many healthcare organizations are beginning to rethink how revenue cycle performance is measured and monitored. Traditional revenue cycle management has focused primarily on claims processing and denial resolution. While these functions remain essential, they address problems only after they occur.
Payment integrity monitoring introduces a more proactive approach. Instead of simply tracking whether a claim was paid, practices evaluate whether the payment amount matches the contracted reimbursement rate. This requires a shift from operational workflows to analytical oversight.
Modern revenue cycle platforms increasingly rely on contract variance analytics, where expected reimbursement amounts are calculated using payer contracts, fee schedules, and CPT level pricing logic. These expected amounts are then compared with the actual payments received from payers.
Automation is essential for this process. Given the volume of claims processed across multiple payers and contract structures, manual reviews cannot reliably detect small discrepancies. By applying automated variance analysis, practices gain the ability to identify underpayments systematically rather than discovering them months later.
How Medetec’s Payment Variance Report Strengthens Revenue Integrity
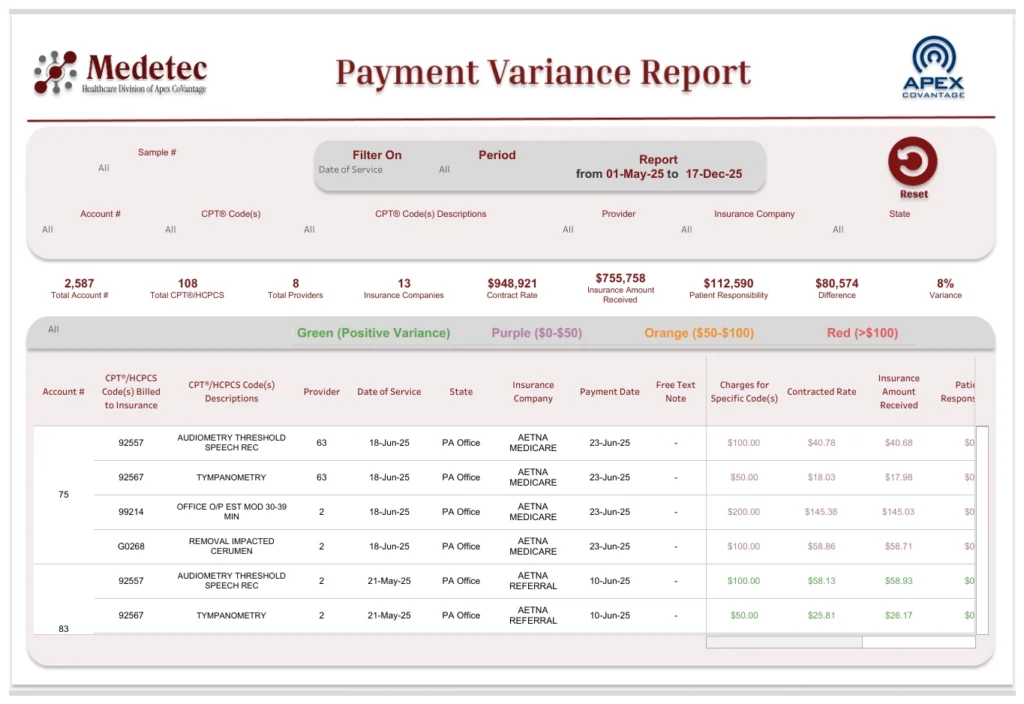
As healthcare organizations move toward payment integrity monitoring, accurate contract intelligence becomes essential. Medetec’s Payment Variance Report was developed to provide that visibility by identifying discrepancies between insurance payments and contracted reimbursement rates.
At the core of this capability is the Payment Variance Database, which calculates the expected reimbursement for each claim using the payer’s fee schedule or contracted rate. The system then compares this expected amount with the actual payment received from the insurer. When differences occur, the variance is automatically flagged for review.
The platform presents this information through a Payment Variance Dashboard that provides encounter level transparency. For each claim, the report displays key data points including the patient account number, CPT or HCPCS codes and descriptions, rendering provider, service location, insurance plan, date of service, and payment date. It also calculates the precise variance between the contracted reimbursement rate and the amount paid by the payer.
By organizing this information in a centralized analytics environment, practices can quickly identify recurring reimbursement discrepancies, detect payer specific patterns, and prioritize recovery opportunities.
Beyond recovering missed revenue, this visibility helps strengthen payer accountability and provides data driven insights that support more informed contract negotiations.
In a Thin-Margin Healthcare Economy, Accuracy Is Strategy
In today’s healthcare environment, protecting revenue requires more than submitting clean claims and resolving denials. It requires verifying that every payment aligns with the terms defined in payer contracts. Without that verification, automated reimbursement systems can quietly introduce small discrepancies that accumulate into meaningful financial loss over time.
For high performing practices, revenue integrity is no longer based on assumptions. It depends on validating every payment against contracted rates and identifying variances before they become long term leakage.
As reimbursement models grow more complex, practices that combine operational efficiency with payment intelligence will be better positioned to protect their margins. Organizations looking to strengthen revenue integrity should begin by understanding where payment variances occur and how those gaps can be systematically addressed.
Explore how Medetec can help your practice quantify and close hidden revenue gaps.